
The American Society of Regional Anesthesia has announced it will be hosting a novel video guided session moderated by Dr Brian Harrington with presenters Eugene Viscusi MD, Edward Mariano MD, and Santhanam Suresh MD. It will feature submitted videos by ASRA members and a Panel Discussion and an Open Forum.
Author: John Gerancher
Night of the Machines hosted by Dr Mike Olympio at Wake Forest University School of Medicine
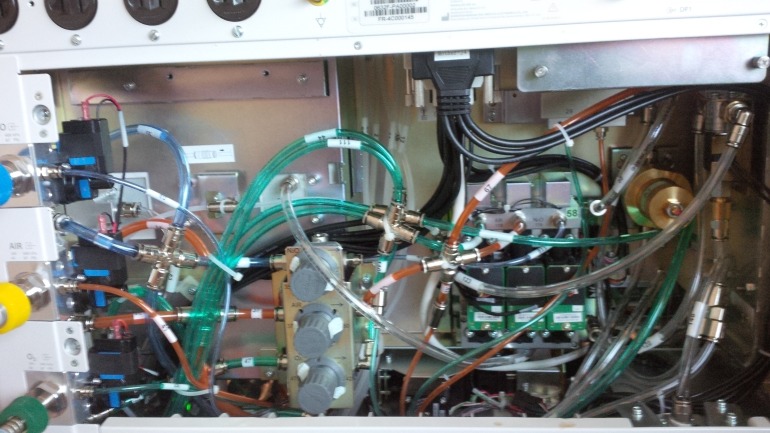
I am grateful for the opportunity to have attended the Anesthesia Machine Workshop “Night of the Machines” put on by Dr Mike Olympio who has done so for about every other year at Wake Forest University School of Medicine. This year’s was held in the Center for Applied Learning and was well attended by anesthesiology residents, the institution’s anesthesia technicians, several student nurse anesthetists, and a few visitors like myself. The 13 hour program was built on break-out sessions of small groups reading and analyzing schematics and diagrams on older machines, presenting their findings, and followed by expert lectures tying classic design to current machine principals. Representatives from anesthesia machine companies such as Mindray and Drager were on hand who presented their companies newest machines–the Mindray A7 and the Perseus A500. The Mindray’s internal components are pictured above. The Perseus has a ventilator powered by a turbine the size of an Oreo cookie that spins at 55,000 rpm. The two day event concluded with a hands-on Datex Aestiva machine pre-anesthesia safety check-out in the simulation laboratory. Participants were challenged to uncover 9 problems laid before them by the author of this course. Dr Olympio provided home baked goods while catered lunch and dinner was enjoyed by all.
What is the “Best” Anesthetic for Oocyte Retrieval
 Pain Relief for Women Undergoing Oocyte Retrieval for Assisted Reproduction (review)
Pain Relief for Women Undergoing Oocyte Retrieval for Assisted Reproduction (review)
Published: January 2013
In: The Cochrane Collaboration
From: EPPI-Centre, University of London
Authors: Kwan I, Bhattacharya S, Knox F, McNeil A.
Review:
In investigating if spinal anesthesia might be the best anesthetic and analgesic approach for oocyte retrieval, I found a recent and complete review on anesthesia and oocyte retrieval. The main result of this review was that use of more than one pain relief modality improved patient comfort. My informal on-line survey of patient information provided for patients by fertility clinics suggests propofol infusion as procedural sedation/general anesthesia is likely the most common method employed for oocyte retrieval in the US.
Original Abstract:
BACKGROUND:
Various methods of conscious sedation and analgesia have been used for pain relief during oocyte recovery in in vitro fertilisation (IVF) and intra-cytoplasmic sperm injection (ICSI) procedures. The choice of agent has also been influenced by the quality of sedation and analgesia as well as by concerns about possible detrimental effects on reproductive outcomes.
OBJECTIVES:
To assess the effectiveness and safety of different methods of conscious sedation and analgesia on pain relief and pregnancy outcomes in women undergoing transvaginal oocyte retrieval.
MAIN RESULTS:
With this update, nine new studies were identified resulting in a total of 21 trials including 2974 women undergoing oocyte retrieval. These trials compared five different categories of conscious sedation and analgesia: 1) conscious sedation and analgesia versus placebo; 2) conscious sedation and analgesia versus other active interventions such as general and acupuncture anaesthesia; 3) conscious sedation and analgesia plus paracervical block versus other active interventions such as general, spinal and acupuncture anaesthesia; 4) patient-controlled conscious sedation and analgesia versus physician-administered conscious sedation and analgesia; and 5) conscious sedation and analgesia with different agents or dosage. Evidence was generally of low quality, mainly due to poor reporting of methods, small sample sizes and inconsistency between the trials. Conflicting results were shown for women’s experience of pain. Compared to conscious sedation alone, more effective pain relief was reported when conscious sedation was combined with electro-acupuncture: intra-operative pain mean difference (MD) on 1 to 10 visual analogue scale (VAS) of 3.00 (95% CI 2.23 to 3.77); post-operative pain MD in VAS units of 2.10 (95% CI 1.40 to 2.80; N = 61, one trial, low quality evidence); or paracervical block (MD not calculable).The pooled data of four trials showed a significantly lower intra-operative pain score with conscious sedation plus paracervical block than with electro-acupuncture plus paracervical block (MD on 10-point VAS of -0.66; 95% CI -0.93 to -0.39; N = 781, 4 trials, low quality evidence) with significant statistical heterogeneity (I(2) = 76%). Patient-controlled sedation and analgesia was associated with more intra-operative pain than physician-administered sedation and analgesia (MD on 10-point VAS of 0.60; 95% CI 0.16 to 1.03; N = 379, 4 trials, low quality evidence) with high statistical heterogeneity (I(2) = 83%). Post-operative pain was reported in only nine studies. As different types and dosages of sedative and analgesic agents, as well as administrative protocols and assessment tools, were used in these trials the data should be interpreted with caution. There was no evidence of a significant difference in pregnancy rate in the 12 studies which assessed this outcome, and pooled data of four trials comparing electro-acupuncture combined with paracervical block with conscious sedation and analgesia plus paracervical block showed an odds ratio (OR) of 0.96 (95% CI 0.72 to 1.29; N = 783, 4 trials) for pregnancy. High levels of women’s satisfaction were reported for all modalities of conscious sedation and analgesia as assessed in 12 studies. Meta-analysis of all the studies was not attempted due to considerable heterogeneity.For the rest of the trials a descriptive summary of the outcomes was presented.
CONCLUSIONS:
The evidence from this review of 21 randomised controlled trials did not support one particular method or technique over another in providing effective conscious sedation and analgesia for pain relief during and after oocyte recovery. The simultaneous use of more than one method of sedation and pain relief resulted in better pain relief than one modality alone. The various approaches and techniques reviewed appeared to be acceptable and were associated with a high degree of satisfaction in women. As women vary in their experience of pain and in coping strategies, the optimal method may be individualized depending on the preferences of both the women and the clinicians and resource availability.
The Assertive Actuary: A Cautionary Tale.. from the ASA Newsletter
Ronald L. Harter, M.D. is Professor and Chair of the Department of Anesthesiology, Ohio State University Wexner Medical Center, Columbus, Ohio. He has authored an insightful editorial in December’s ASA Newsletter in his capacity as  Vice Speaker, ASA House of Delegates on professional assertiveness for anesthesiologists. After introducing the topic by way of the self-deprecating humor of an actuary friend of his, he urges us to “embark boldly into … new territory, keeping one foot firmly planted in the O.R., while we stride further into peri-operative leadership.” The line that caught my eye: “The spectrum of acute pain management options we offer our patients has never been broader, and our skill and expertise at ultrasound-guided regional nerve blocks frequently allows earlier patient discharge and results in high levels of satisfaction for our patients.”
Vice Speaker, ASA House of Delegates on professional assertiveness for anesthesiologists. After introducing the topic by way of the self-deprecating humor of an actuary friend of his, he urges us to “embark boldly into … new territory, keeping one foot firmly planted in the O.R., while we stride further into peri-operative leadership.” The line that caught my eye: “The spectrum of acute pain management options we offer our patients has never been broader, and our skill and expertise at ultrasound-guided regional nerve blocks frequently allows earlier patient discharge and results in high levels of satisfaction for our patients.”
Redefining Roles in the Changing Landscape of HealthCare
 Anesthesiology News in December 2014 includes a thoughtful editorial by current CA-2 Anesthesiology resident, Michael DeCicca M.D., of the State University of New York Upstate Medical Center in Syracuse New York. It is an excellent characterization of the tension between CRNA’s and anesthesiologists as well as a good reminder of what it means to be a “Luddite”. To further our chosen profession, Dr DeCiccia asks us potential Luddites to “consider the reasons (we) went into anesthesia in the first place,the facets of the specialty that piqued (our) interest, and develop them.”
Anesthesiology News in December 2014 includes a thoughtful editorial by current CA-2 Anesthesiology resident, Michael DeCicca M.D., of the State University of New York Upstate Medical Center in Syracuse New York. It is an excellent characterization of the tension between CRNA’s and anesthesiologists as well as a good reminder of what it means to be a “Luddite”. To further our chosen profession, Dr DeCiccia asks us potential Luddites to “consider the reasons (we) went into anesthesia in the first place,the facets of the specialty that piqued (our) interest, and develop them.”
